
From the Family Health Manager to the Family Health Agent: HealthVault 2030
How a forgotten HealthVault insight about households, delegated care, and the real operating unit of healthcare points toward the next platform in the industry.
This essay is going to take a minute. If you don’t have the time right now, bookmark it and come back when you do. I want to trace a line from one of the deepest insights behind HealthVault — that healthcare is usually managed not by “the patient” in isolation, but by a Family Health Manager inside the household — to a category I now think AI makes possible: the Family Health Agent. To do that, I need to move from field research in Midwestern kitchens to delegated records, HIPAA, Google Health, Josh Mandel’s infrastructure warnings, and the uncomfortable but unavoidable question of who actually pays for coordination in a system built on fragmentation. I’ll explain the jargon when I use it. I’ll try to be concrete about where I think the business starts. And I’ll also be honest about the parts that are still unresolved, because there are some very real ones.
TL;DR: When we built HealthVault, the deepest insight was not that patients needed their records online. It was that healthcare is usually managed by a Family Health Manager inside the household — the person who keeps track of appointments, medications, forms, follow-ups, and all the dropped tasks the system quietly leaves behind. HealthVault captured that reality with delegated, patient-controlled records. The next step is the Family Health Agent: a patient-authorized system that manages the same role in software, absorbing the administrative entropy of care across fragmented institutions. The business opportunity is not selling more dashboards to patients. It is reducing coordination failure for the plans, providers, pharmacies, and navigation programs that already pay for it.
This is a category thesis for health-tech builders, operators, investors, and policy people who think the next platform in healthcare may emerge not from the chart or the claim, but from the role that has been quietly holding the system together all along.
Sealab 2020 and the futures we actually got
 One of my favorite cartoons as a kid was Sealab 2020. Not the later Adult Swim spoof Sealab 2021, which was magnificently deranged in the way only Adult Swim can be, but the earnest original: scientists living in an undersea base, peering through giant windows into the abyss, confidently occupying a future that seemed both inevitable and properly overengineered. It ran for a single season, but childhood has a way of turning thirteen episodes into an epoch, and in my memory Sealab 2020 lasted approximately as long as the Roman Empire. The funny thing, of course, is that the future almost never arrives where you expect it. We did not get undersea cities or moon hotels, and we barely got the sort of space station that 2001 seemed to regard as an administrative inevitability. What we got instead was the network, the smartphone, and now AI systems capable of moving information, intent, and action across institutions that still behave as though the fax machine was not just viable, but spiritually correct.
One of my favorite cartoons as a kid was Sealab 2020. Not the later Adult Swim spoof Sealab 2021, which was magnificently deranged in the way only Adult Swim can be, but the earnest original: scientists living in an undersea base, peering through giant windows into the abyss, confidently occupying a future that seemed both inevitable and properly overengineered. It ran for a single season, but childhood has a way of turning thirteen episodes into an epoch, and in my memory Sealab 2020 lasted approximately as long as the Roman Empire. The funny thing, of course, is that the future almost never arrives where you expect it. We did not get undersea cities or moon hotels, and we barely got the sort of space station that 2001 seemed to regard as an administrative inevitability. What we got instead was the network, the smartphone, and now AI systems capable of moving information, intent, and action across institutions that still behave as though the fax machine was not just viable, but spiritually correct.
That turns out to matter a great deal in healthcare, because healthcare has never really suffered from a lack of information so much as a lack of coherent movement between islands of information. Hospitals, specialists, labs, payers, pharmacies, and family members all know different parts of the story, but the system as a whole has spent decades behaving as though assembling those fragments into something usable were somebody else’s problem — ideally somebody underpaid, sleep-deprived, and already on hold with an insurer. When we started building HealthVault, that was the problem we were really trying to solve. The insight that made the product different was not just technical, and it certainly was not merely a prettier way to store PDFs. It was a shift in where we thought the center of gravity actually was.
The first Copernican shift in healthcare software
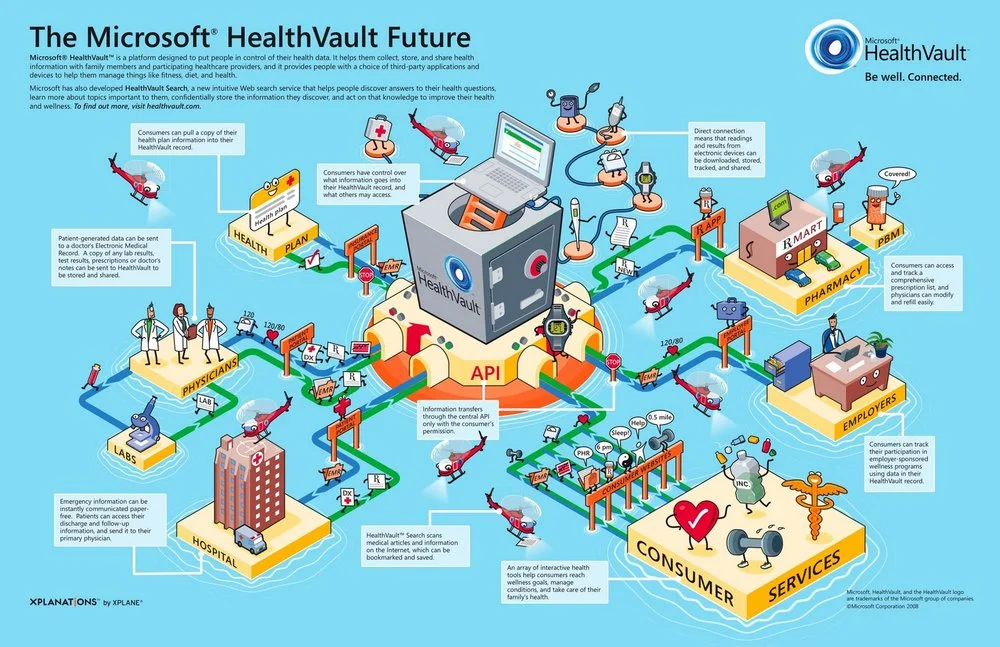
![]() When Peter Neupert launched HealthVault, the line we used was that “the family is the center of healthcare.” I should probably note, once and only once, that I wrote that line in Peter’s speech. But the reason it landed had very little to do with rhetoric and everything to do with the research. By then, we had already spent months studying how healthcare actually worked inside households, and the conclusion was difficult to miss once you saw it. If you want to inspect the public artifact, Peter’s launch remarks are still worth reading, because they capture the public expression of a much deeper product thesis than most people realized at the time.
When Peter Neupert launched HealthVault, the line we used was that “the family is the center of healthcare.” I should probably note, once and only once, that I wrote that line in Peter’s speech. But the reason it landed had very little to do with rhetoric and everything to do with the research. By then, we had already spent months studying how healthcare actually worked inside households, and the conclusion was difficult to miss once you saw it. If you want to inspect the public artifact, Peter’s launch remarks are still worth reading, because they capture the public expression of a much deeper product thesis than most people realized at the time.
Peter had hired me quite deliberately for that job. He did not want only someone from the healthcare establishment, fully steeped in its assumptions and acronyms, though God knows the industry never suffers from an undersupply of acronyms. He wanted someone who could blend consumer research with technology thinking, which happened to line up rather neatly with my own background: nearly a decade at Procter & Gamble learning how households actually behave, followed by another stretch in technology companies trying to build systems that could scale. So instead of beginning with a conference room full of experts explaining how healthcare ought to work, we started by observing how it actually worked.
We brought in a research team I had worked with for years and asked them to spend time with families over several months, not just dropping in for a tidy interview but watching the real logistics of care management unfold in the wild. What they found was almost embarrassingly obvious once you saw it. Healthcare was rarely managed by “the patient” in isolation. More often than not, it was coordinated by someone inside the household who quietly carried the operational burden for everyone else: tracking appointments, remembering medication changes, dealing with insurance forms, keeping the immunization records straight, and making sure the right information arrived at the right doctor at the right time. We started calling that person the Family Health Manager. Usually it was mom, though certainly not always. The point was the role, not the gender. Once you saw that pattern, a great many personal health records suddenly looked as though they had been designed around the wrong center of gravity.
What the families taught us
 The thing I remember most vividly from that field work is how little any of it resembled the clean boxes on healthcare PowerPoints. You did not need a white paper once you had spent a few afternoons in Midwestern kitchens and family rooms. Somewhere between the half-sorted school forms, the bottle of children’s acetaminophen, the insurance EOB that appeared to have been drafted by Kafka’s least cheerful nephew, and the pediatrician’s after-hours number written on an index card in increasingly urgent handwriting, the whole theory of the product would reveal itself. Every household seemed to contain a stack of forms reproducing quietly by mitosis on the countertop, which I realize is not a medically approved reproductive pathway, but it certainly appeared to be the dominant one, and one person — again, often mom, but not always — serving as the unpaid systems integrator for the entire family. The official story in healthcare IT was always patient, provider, chart. The actual story was calendar, caregiver, chaos.
The thing I remember most vividly from that field work is how little any of it resembled the clean boxes on healthcare PowerPoints. You did not need a white paper once you had spent a few afternoons in Midwestern kitchens and family rooms. Somewhere between the half-sorted school forms, the bottle of children’s acetaminophen, the insurance EOB that appeared to have been drafted by Kafka’s least cheerful nephew, and the pediatrician’s after-hours number written on an index card in increasingly urgent handwriting, the whole theory of the product would reveal itself. Every household seemed to contain a stack of forms reproducing quietly by mitosis on the countertop, which I realize is not a medically approved reproductive pathway, but it certainly appeared to be the dominant one, and one person — again, often mom, but not always — serving as the unpaid systems integrator for the entire family. The official story in healthcare IT was always patient, provider, chart. The actual story was calendar, caregiver, chaos.
And families, of course, are not static. Children turn eighteen and the access rules change. Parents age into needing help themselves. Couples divorce. Grandparents move in. Someone develops cognitive decline and responsibility shifts to an adult child. Someone dies, which is heartbreaking in the human sense and administratively clarifying in the grimmest possible way, because nothing reveals the true design of a system faster than asking who is still allowed to do what after the worst has happened. The old PHR model — one patient, one record, one owner — could not really metabolize that reality because it had started from the wrong cosmology. It assumed healthcare was an interaction between an individual and an institution. The field work told us something messier and, in my view, much more useful: healthcare is managed inside a changing household, by delegated authority, under conditions of permanent mild confusion.
That was the original Copernican shift of HealthVault. We did not move the patient out of the picture. We moved the model closer to reality. The patient still mattered, obviously. But the patient was not the only operational unit in the system, and often not even the primary one. The real unit of care was the household, usually organized around a Family Health Manager and whatever delegated helpers happened to be carrying responsibility at the time. Healthcare, in other words, was being run on a household operating system nobody had bothered to model. Every family has at least one person who knows where the forms are buried.
How Sean Nolan turned insight into architecture
This is the part of the story that can get flattened if you tell it too quickly. The Family Health Manager insight was not just a marketing observation. It became architecture because Sean Nolan immediately understood what it implied for the platform. Sean and I ran HealthVault two-in-a-box: I handled the go-to-market side, Sean ran the technology platform, and one of the pleasures of that partnership was that when a piece of user insight surfaced, he could often see the structural consequence faster than anyone else in the room.
Most personal health records at the time assumed a fairly simple world: one patient, one record, one owner. But that model falls apart the moment you place it inside a real household. So Sean built something different. HealthVault supported multiple records, multiple levels of sharing, delegated custodianship, and transfer of responsibility as family circumstances changed. If you want to see that design logic in its own native habitat, it shows up very clearly in Microsoft’s old HealthVault Application Integration Recommendations, in the support guidance for sharing a HealthVault record, and in the old HealthVault Service Specification. The product did not treat caregiving as a feature. It treated caregiving as part of the underlying object model.
There was a quiet legal elegance to that model as well, and any serious 2030 version has to preserve it. One of the reasons the original HealthVault architecture mattered was that once the record was under the patient’s control, the patient could authorize where it went. That lined up neatly with rights HIPAA already recognizes: individuals have the right to access and obtain copies of their PHI, direct a covered entity to send that information to a designated third party, and rely on a personal representative to act on their behalf within the scope of the relevant authority. If you want the current source material, HHS lays this out in its guidance on Individuals’ Right under HIPAA to Access their Health Information and Personal Representatives. Healthcare has many theological disputes; this one at least comes with statutory guidance. That mattered then, and it matters even more now, because the future version only works if it remains patient-controlled, family-delegated, auditable, and permissioned all the way down. Otherwise you do not have a care platform. You have a compliance incident with a pleasant onboarding flow.
Google Health as the control group
![]() Google is useful here not as a punching bag but as a control group. When Google launched Google Health in 2008, the framing was unmistakably about the individual gathering and managing his or her own record online. You can see that in Marissa Mayer’s “Google Health, a first look”, and you can see the same framing in contemporary coverage like Wired’s “Google Launches Medical Records App”. That was a perfectly reasonable place to start if you believed the atomic unit of the system was the solitary patient with a solitary record. In fairness, most of the industry believed exactly that.
Google is useful here not as a punching bag but as a control group. When Google launched Google Health in 2008, the framing was unmistakably about the individual gathering and managing his or her own record online. You can see that in Marissa Mayer’s “Google Health, a first look”, and you can see the same framing in contemporary coverage like Wired’s “Google Launches Medical Records App”. That was a perfectly reasonable place to start if you believed the atomic unit of the system was the solitary patient with a solitary record. In fairness, most of the industry believed exactly that.
What makes the comparison interesting is that you can watch Google discovering the same reality we had stumbled onto earlier. In 2009, Google published “Google Health: helping you better coordinate your care”, which is a revealing title because the problem has suddenly widened from “my record” to “the care of loved ones.” But the product expression of that discovery was still essentially a sharing model layered on top of an individual record worldview. Caregiving appeared as an extension. In HealthVault, by contrast, delegated management had already become a native concept in the system. That sounds like a subtle difference until you live with it for a while, at which point it turns out not to be subtle at all. In healthcare software, permissioning is architecture. It is the difference between adding a guest room and realizing, somewhat late in the renovation, that the family actually lives in the kitchen.
By 2011, Google posted its shutdown note, saying the service was not having the broad impact it had hoped for, even though it had developed a loyal following among health and wellness enthusiasts, and among tech-savvy patients and caregivers. I do not think the correct lesson is “Microsoft good, Google bad.” That is too shallow to be useful, and besides, triumphalism ages even worse than software. The better lesson is that both companies were grappling with the same underlying reality, but one of them discovered caregiving as a feature request while the other let it reshape the data model. One added another epicycle. The other moved the sun.
Why HealthVault was early, not wrong
If you want the best retrospective account of why HealthVault now looks more plausible than it did when we launched it, Sean’s later writing is still the place to go. His essays “Health IT: More I, less T”, “SMART Part 4: Healthcare data sucks, and FHIR is no exception”, “explain my notes”, and “Refine your search for ‘gunshot wound’” form a kind of accidental archive of the long arc here. Sean makes two points in particular that are worth preserving. First, healthcare data is story-shaped before it is schema-shaped. Second, “comprehensive messy data trumps spotty clean data” far more often than tidy software people would prefer. Both observations were true in the HealthVault era. They are, if anything, more true now.
What has changed is that the rails are finally real. FHIR is no longer a standards-body hobby; SMART App Launch gives applications a workable model for launch and authorization; and patient-mediated access, payer APIs, and prior-auth workflows now have enough institutional backing to matter. None of that means healthcare interoperability has become elegant, and I would caution against getting drunk on a standards deck. FHIR did not descend from Sinai, but at least now there are tablets. What matters is that the world is no longer empty. The original HealthVault insight was right before the infrastructure could really carry it.
What Josh Mandel is seeing in the rails
If Sean’s writing helps explain why HealthVault was early, Josh Mandel’s recent work helps explain what kind of future might finally make the next version possible. Josh is one of the most useful guides here because he is not just opining from the cheap seats. He is a physician and software engineer who, in his current role at Microsoft Research, has spent years working on frictionless data access, authorization, analytics, and app integration. In other words, he is one of the people who have spent years trying to make the rails real.
My summary of Josh’s recent thinking is this: the standards are finally real enough to build on, but the real bottlenecks have shifted from representation to authorization, orchestration, scale, and access economics. In “Designing for Delay”, he makes the point that clinical workflows like prior authorization, trial matching, and specialty consult coordination are inherently asynchronous. They do not happen instantly. They stretch across time, actors, and institutions. Prior authorization, in particular, is a perfect example of the category: too structured to remain pure phone-tag forever, too messy to be solved by a static form flow, and exactly the sort of thing a Family Health Agent should manage relentlessly on behalf of the household. In “Authorization as a Network Scaling Problem”, he argues that the hard part is no longer getting OAuth scopes onto a slide; it is the fact that the real authorization logic still lives in site-specific configurations that do not travel across networks. In his piece on patient-directed notifications, he outlines a “provider-affirmed routing” model that preserves provider control while still allowing network-level scale. In “The Battle for Health Data Moves to the Fine Print”, he makes the point that as the technical doors open, the bottleneck moves into contracts, fees, indemnities, and access terms. And in “7,000+ Clicks to Register a FHIR App” and the follow-on Health Skillz work, he shows just how rough the developer reality still is even when the standards exist on paper.
This matters enormously for the Family Health Agent thesis, because it tells us what the product is not. It is not a magical future system that waits for every provider, payer, pharmacy, and vendor to become fully agent-native before it becomes useful. It is an overlay that has to operate across the messy non-agent stack we actually have: portals, prior-auth APIs, brittle SMART registrations, pharmacy workflows, brokered notifications, and all. The point is not to bypass standards altogether. The point is to bypass the fantasy that every actor in the system must first agree on one ontology, one workflow, and one legal posture before coordination can improve.
That is where Josh’s work and this essay converge. He is mapping the rough, uneven rails that are emerging. I am proposing a role-native product that can ride those rails without waiting for them to become perfect. If HealthVault was about delegated, patient-controlled records, the next move is a system that can actually manage the delegated work on top of the infrastructure we now have. The next question is what kind of coordination system can create value on top of those rails even before they become elegant.
The second Copernican shift: coordination without consensus
 This is where Sangeet Paul Choudary becomes important. If you have not followed his work, Sangeet is one of the sharper thinkers on how platforms and AI reshape industries, and his recent writing has been especially helpful in naming what may actually be changing. The key idea is not just that AI automates tasks. It is that AI lowers the cost of translation and coordination across fragmented actors who do not share the same systems, incentives, or mental models. In his recent HBR piece and his broader Reshuffle writing, he argues that when those coordination constraints change, the architecture of an industry changes with them. That is a very interesting lens for healthcare, because healthcare is basically a giant machine for testing whether coordination can happen without consensus.
This is where Sangeet Paul Choudary becomes important. If you have not followed his work, Sangeet is one of the sharper thinkers on how platforms and AI reshape industries, and his recent writing has been especially helpful in naming what may actually be changing. The key idea is not just that AI automates tasks. It is that AI lowers the cost of translation and coordination across fragmented actors who do not share the same systems, incentives, or mental models. In his recent HBR piece and his broader Reshuffle writing, he argues that when those coordination constraints change, the architecture of an industry changes with them. That is a very interesting lens for healthcare, because healthcare is basically a giant machine for testing whether coordination can happen without consensus.
The first Copernican shift of HealthVault was to realize that the patient-provider dyad was not the real operating unit of care. The second is to realize that the Family Health Manager does not have to remain a purely human bottleneck forever. Once software gets good enough at translation, memory, orchestration, and permissions, the role itself becomes amenable to a new kind of system. Not a doctor in software. Not a generic chatbot floating above the system. A manager for a role that has historically required one overwhelmed human after another.
That is why I think “coordination without consensus” is the better frame than “let’s wait for healthcare standards to save us.” Standards matter. They matter a lot. But the next wave of value may come from software that uses standards where they exist, works around them where they don’t, and relentlessly manages the handoffs in between.
From the Family Health Manager to the Family Health Agent
 Start with the name. By Family Health Agent, I do not mean an artificial doctor. The world does not need a large language model in a lab coat with the bedside manner of Clippy. I mean something much more practical and, to my mind, much more valuable: a software chief of staff for the Family Health Manager and the household they manage. A patient-authorized, family-delegated system that can coordinate records, permissions, follow-ups, medications, summaries, handoffs, and administrative tasks across the household without pretending that every institution in the chain has suddenly become modern, interoperable, and spiritually well. The point is not to erase the human role. The point is to give that human role a new operating layer. Mom has been the middleware for long enough.
Start with the name. By Family Health Agent, I do not mean an artificial doctor. The world does not need a large language model in a lab coat with the bedside manner of Clippy. I mean something much more practical and, to my mind, much more valuable: a software chief of staff for the Family Health Manager and the household they manage. A patient-authorized, family-delegated system that can coordinate records, permissions, follow-ups, medications, summaries, handoffs, and administrative tasks across the household without pretending that every institution in the chain has suddenly become modern, interoperable, and spiritually well. The point is not to erase the human role. The point is to give that human role a new operating layer. Mom has been the middleware for long enough.
One way to see the opportunity more clearly is to recognize that some roles in the world are not primarily expert roles so much as managerial ones. They require memory, follow-through, escalation, pattern recognition, and a refusal to let important things quietly fall on the floor. The Family Health Manager is exactly that kind of role. It is managerial labor performed under emotional stress, across fragmented systems, with terrible tooling, high stakes, and a depressing amount of hold music. That is precisely the sort of role where a really great manager in software starts to look less like a gimmick and more like relief.
A Family Health Agent is not just a chatbot with better manners. It requires a new set of primitives. It needs a Household Health Graph to model who is involved in a person’s care and how those relationships change over time. It needs a Delegation Ledger to track who can act for whom, under what authority, and in which contexts. It needs a Consent Engine to manage permissions, revocations, transitions at age eighteen, powers of attorney, and all the other delightful surprises life throws at household administration. And it needs a Longitudinal Care Timeline to keep the actual story coherent across providers, plans, pharmacies, labs, and family members. Once you start naming the primitives, the category stops sounding like metaphor and starts sounding like product.
The value of that product is not that it sounds intelligent in a demo. It is that it behaves like a tireless manager of a role that has historically required one exhausted human after another. It checks what has been dropped. It notices what changed. It follows up every day until the prior authorization is granted. It moves the prescription from Washington to California when the family is traveling. It remembers that the specialist wanted the lab repeated in two weeks and notices that nobody actually booked the follow-up. It recognizes that “pending” is often just a polite administrative synonym for “forgotten.” In other words, it absorbs the entropy of the system so the household does not have to.
The human role does not disappear. The Family Health Agent does not eliminate the Family Health Manager; it changes the job from full-time coordinator to supervisor, exception handler, and final authority. The goal is not to remove the human from the loop. It is to stop requiring the human to be the loop. The goal is not autonomy for its own sake. The goal is to reserve human energy for judgment, consent, and care instead of clerical persistence.
A useful way to make that concrete is to look at Heydex, which positions itself as an AI chief of staff. Right now the product is pitched in the language of productivity, which makes sense; “chief of staff” is a polite way of saying that your current operating system consists of memory, tabs, calendar invites, and the rising suspicion that something important has already fallen off the back of the truck. But imagine the same core idea pointed at the household health graph rather than the knowledge worker’s calendar. Suddenly the Family Health Manager has software assistance that actually resembles the work being done: notice the cardiology follow-up never got booked, assemble the prior-auth packet, keep track of the refill gap, summarize what the nephrologist actually needs before the visit, and ask the right human for the right permission when the kid turns eighteen or Grandpa’s power of attorney changes. In that world, Heydex stops looking like a productivity tool and starts looking like an early prototype of a healthcare asset.
In pediatrics, that means helping a family transition gracefully when a child ages into adulthood instead of dropping everyone through a bureaucratic trap door. The parent who has spent fifteen years managing asthma meds, immunization records, sports forms, and specialist visits should not wake up on the wrong side of an eighteenth birthday and suddenly become a stranger to the system.
In eldercare, it means turning the adult daughter from unpaid ETL pipeline into actual daughter again. She should not have to be the one reconciling medication lists across three portals, explaining last week’s hospitalization for the fourth time, and discovering by accident that the follow-up never got scheduled because everyone assumed somebody else was handling it.
In oncology, it means recognizing that a care journey is not a chart plus a claim plus a pharmacy event; it is a cross-institutional relay race whose baton has been dropped far too many times. The Family Health Agent should know that the missing prior-auth packet, the delayed specialty-pharmacy outreach, and the absent lab result are not separate clerical inconveniences. They are the care journey.
How the Family Health Agent actually works
The easiest way to understand the Family Health Agent is not as a chatbot, but as a role-specific control loop. It begins with authority. The patient — and, where appropriate, the Family Health Manager or other delegated helper — connects the relevant records, defines who can act for whom, and sets the boundaries of what the system is allowed to do. That gives the agent its working surface: not “all the data,” but the subset of records, permissions, and tasks it is authorized to manage.
From there, the Family Health Agent builds a longitudinal working memory of the household’s health activity. Not just a pile of records, but a live timeline of appointments, medications, prescriptions, labs, prior-auth states, follow-ups, referrals, deadlines, and unresolved tasks. The point is not to recreate the chart. The point is to create an operational view of what is supposed to happen next, what has already happened, and what looks as though it may have been dropped.
Once that state exists, the agent starts doing managerial work. It checks whether the prior authorization was actually submitted. It notices that the refill was requested but never filled. It sees that the lab was ordered but not scheduled, or scheduled but not completed, or completed but never surfaced to the right person. In other words, it manages the backlog of care.
It then acts within bounded authority. If it is allowed to draft a packet, it drafts the packet. If it is allowed to move a prescription, it prepares the transfer. If it can schedule or re-confirm an appointment, it does so. If it needs human approval, it asks. If it needs to notify the Family Health Manager that something slipped, it does that. The system is not “autonomous” in the sci-fi sense. It is persistent in the managerial sense. Think less HAL 9000, more the world’s most conscientious case manager with perfect memory and zero resentment.
The most important thing it does is re-check. It does not assume that one action resolved the problem. It follows up. It notices that “pending” has become “forgotten.” It notices that a denial requires an appeal. It notices that the patient is now traveling in another state and the original plan no longer works. This is where the Family Health Agent earns its keep: not in one brilliant act of diagnosis, but in relentless, bounded, administratively competent follow-through.
The human remains in charge. The Family Health Manager becomes the supervisor, exception handler, and final authority instead of the full-time transport layer for the entire system. The point is not to replace care. The point is to stop requiring a human being to perform unpaid systems integration just to keep care from falling apart.
Where the $5.3 trillion goes — and who should actually pay
If you are going to propose a new platform category inside healthcare, you should probably start by looking at where the money actually goes. U.S. healthcare spending reached $5.3 trillion in 2024, or $15,474 per person, representing 18.0% of GDP. By type of service, the biggest buckets were hospital care at about $1.6 trillion and 31% of total spending, physician and clinical services at about $1.1 trillion and 21%, and retail prescription drugs at $467 billion and 9%. By source of funds, private health insurance accounted for 31% of spending, Medicare 21%, and Medicaid 18%. If you want the simplest possible read on the economics, it is this: the biggest dollars in healthcare are still being burned in hospital and physician spending, financed primarily by private insurance and government programs.
One rough way to map this to Jensen Huang’s favorite AI stack language is to think of healthcare as a layered system. Biology and patients are the substrate. Diagnostics, notes, claims, and devices are the data-capture layer. EHRs, prescriptions, prior-auth systems, portals, and payer APIs are the transaction rails. The Family Health Manager today — and the Family Health Agent tomorrow — is the coordination layer. And the value-capture layer is whoever makes or saves money when coordination failure drops. If you start from that frame, the long-run economic winner is not hard to spot: it is the part of the system already paying for avoidable utilization, abandoned therapy starts, delayed follow-up, administrative overhead, and all the quiet wreckage that follows from dropped tasks.
At system scale, that means payers and risk-bearing provider organizations are the biggest economic beneficiaries. Private insurers, Medicare Advantage plans, Medicaid managed care, ACO-like entities, and integrated delivery systems are the ones directly exposed when poor coordination turns into admissions, readmissions, no-shows, disease progression, or generic administrative waste.
But GTM is not the same thing as macroeconomics. If I were starting this company tomorrow, I would not begin with a consumer subscription and I would not begin by trying to boil the ocean inside Epic. I would start in specialty therapy access — oncology, immunology, neurology, rare disease — because that is where coordination failures are most explicit and where budgets already exist for benefits investigation, prior authorization support, hub enrollment, adherence outreach, refill management, and the whole swampy managerial layer between prescription and therapy start. The specialty pharmacy literature makes this very plain: pharmacists and support teams already conduct benefits investigations, obtain insurance approval and appeals, submit hub enrollment forms, route the prescription to the right specialty pharmacy, help patients enroll in copay assistance, and then monitor adherence and safety labs after therapy begins. The National Council for Prescription Drug Programs is equally explicit that hub services are manufacturer-sponsored programs supporting access, affordability, and adherence. In other words: the system is already paying for the role. It is just paying for it badly, manually, and in fragments.
That is the business case in one sentence: the Family Health Agent does not need a miraculous new budget. It needs to cannibalize an old one.
More specifically, it should replace, or at least sharply reduce, spend on fragmented call-center labor, outsourced navigation vendors, repetitive prior-auth follow-up work, manual benefits investigation, hub-service overhead that exists only because every handoff is brittle, and generic care-management outreach that spends half its life rediscovering what was dropped the week before. The first buyer is whoever is already paying humans and vendors to do coordination badly, expensively, and over and over again.
Start where the coordination work is explicit and the ROI is easy to measure. Then move up into the layer that absorbs the biggest dollars when coordination failure spills into hospital and physician spend. That is also where diagnostics and data-rich players like Labcorp become strategically interesting. Longitudinal household-managed data is clearly valuable for patient identification, recruitment, evidence generation, market access, and therapy optimization. But I would treat that as act two, not the first commercial wedge. Act one is replacing manual coordination labor where it is already funded.
Why the incumbents are badly positioned to own it
One of the reasons this feels like a real category and not just a good metaphor is that the obvious incumbents are all badly shaped for it. EHR vendors are optimized for institutional workflow, clinician documentation, and billing-adjacent process control; they see the chart brilliantly, but not the household delegation graph. Payers are optimized for adjudication, utilization management, and reimbursement logic; they see the claim, but not the lived choreography of care across the household. Pharmacies see medication workflow, which matters enormously, but they do not see the whole household story either. And consumer health apps, for all their energy, usually start from the lone motivated individual with a dashboard, which is precisely the simplifying assumption the original HealthVault research taught us to distrust.
There is also a more pointed way to say this. The last cycle of health IT poured billions into systems optimized for institutional records and workflow. Epic alone reported $5.7 billion in 2024 revenue. Very little of that spend went to the role that was actually holding fragmented care together inside the household. The industry spent heavily on the chart. It spent comparatively little on the person reconciling the chart with reality.
That leaves a gap, and gaps like this are where platform categories come from. The Family Health Agent sits in the space between institutional systems, family systems, delegated authority, and longitudinal coordination. It is not trying to replace the chart, the claim, the prescription, or the visit. It is trying to make those things hang together inside the household that actually experiences them.
The next platform in healthcare
If this is right, then a depressing amount of the last two decades of healthcare IT has been powerful industries competing around partial views of the system. The chart, the claim, and the consumer app were all important abstractions. None of them was the role actually holding fragmented care together. Care is coordinated inside a changing household by someone carrying delegated authority, household context, and an exhausting amount of memory. That person has historically been a spouse, a parent, an adult child, or some other Family Health Manager. The next great care platform will be built for that role.
And that is why the category claim is stronger than it first sounds. The winning agents in healthcare will not be the ones that posture as disembodied experts floating above the system. They will be the ones that manage a hard, messy, indispensable role better than the system currently allows any human to manage it. The next platform in healthcare will not be an EHR, because EHRs were built for institutions, and it will not be a payer network, because payer networks were built to adjudicate reimbursement. It will be the system that understands the household graph, the delegation graph, the permission graph, and the care timeline well enough to absorb the coordination labor families have been doing by hand for generations. Or, to put it a little less politely: the patient was never the problem. The patient was the workaround. The next platform in healthcare will be the Family Health Agent.
If the category thesis feels directionally right, I’ve taken the liberty of sketching out how the Family Health Agent could actually be built — from product primitives to v1 workflows to a sequence of Claude Code prompts — in a companion post: How to Build the Family Health Agent.
P.S. My friend Peter Frishauf (Founder, Medscape) took a look at an earlier draft of this essay and made a great observation about one important player I largely left out of this essay: Apple. They’re probably not the first budget owner for the Family Health Agent; the first dollars still come from the part of the system already paying for coordination failure. But Apple may be the most important platform layer beneath it. The company now has more than 2.5 billion active devices in market, already treats the Health app as a central, secure place for personal health data, supports sharing Health app data with providers, and has opened its on-device foundation models to developers. If the Family Health Agent becomes real, I would not be surprised if the first buyers are payers, providers, pharmacies, and manufacturer hub programs — and the first truly scaled consumer substrate is Apple. The plans may fund the first wedge. Apple may end up owning the edge.
Acknowledgements
Gratitude to Sean Nolan and Peter Neupert, who reviewed earlier versions of this post and contributed significantly to sharpening it and improving the logic.